







eHealth and the silo culture of medicine

In February SBS Insight broadcast Saving Health. If you missed it, it is worth watching given recent Medicare funding discussions.
As a patient seeing multiple health professionals and having registered, in great hope, for eHealth, I was very interested to hear the doctors thoughts about their own profession. I understood the patients’ perspectives all too well.
There was a general consensus from the medical personnel about the silo culture of medicine in this country. As Dr Ranjana Srivastava said (in relation to repeat testing), “when doctors work in silos, you kind of don’t want to get into other people’s way”: we see this in many walks of life, not just medicine. Dr Charlotte Hespe spoke about the difficulties of getting results across barriers of fragmented communication, Dr Nick Bretland spoke of having to fax (yes, fax) forms to a public hospital to get x-ray results. I had an MRI and the films were available on my smartphone 5 minutes after the scan. Yet the GP has to fax forms to get the results? Bureaucratic red tape forms many of those barriers.
Professor John Dwyer stated ” … we do not have a patient focused health care system.” Assoc. Prof. Terry Hannan of Launceston General Hospital said, “patient centred care is the patient having their own record.”
This is where eHealth comes in. Two people in the studio audience had signed up for eHealth. TWO! Once I discovered I was unwell, I signed up for eHealth. The driver for my doing so was a very embarrassing discussion with my gastroenterologist.
“Have you had a colonoscopy before?”
“Yes, I have, years ago.”
“Who did it?”
“Ummmm, I’ve forgotten.”
“Where did you have it done?”
“Ummmm, I’ve forgotten.”
eHealth would solve that problem, nicely, wouldn’t it?
Not so much. Watching the above Insight episode, I learnt I actually have to have my GP upload some sort of summary, and according to Dr Bretland he had initially had to fill out paper forms to send in to establish his patients’ eHealth records. That will explain the scanty nature of my own eHealth record – I’ve not discussed it with my GP at all.
Candice Kriewaldt, a patient with rheumatoid arthritis, spoke of having to navigate the system herself and collate her own medical record. She highlighted the difficulties of getting medical records from one specialist to pass on to a new specialist and the problems that lead to in her treatment. I do exactly the same as Candice. I have a pretty pink folder I carry around with pathology requests pending, results, imaging CDs and details of medications.
The programme makes it reasonably clear the medical profession in Australia is still very paper based, despite the availability of technology. It appears some 4% of Australian’s surveyed expressed concerns about privacy, so eHealth is not yet where it could be or should be. May I suggest we let the 4% opt-out if they so wish and let the rest of us have our eHealth fully functional!
Here is a screen shot from my eHealth record.
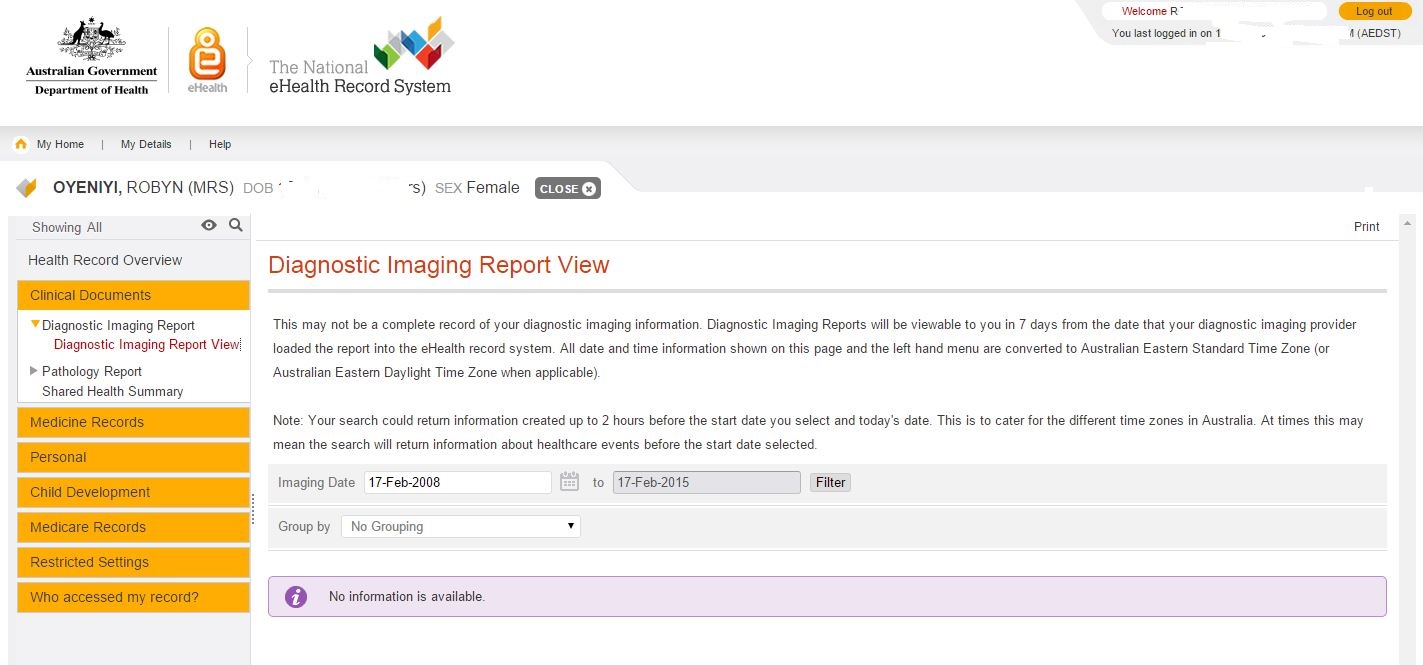
No data about my MRI
The eHealth website says:
Your eHealth record allows you and your doctors, hospitals and other healthcare providers to view and share your health information to provide you with the best possible care.
I had taken “share your health information” to mean all my recent scans and blood test results would be there. After all, I had scans available on my mobile phone five minutes after I had the scans! Surely they would be on the big fancy new eHealth web site? Well, actually, no, they are not there. I dug a little deeper into the FAQs (that means Frequently Asked Questions for the uninitiated) and found out why.
It is expected that you may start to see your pathology and diagnostic imaging reports in your eHealth record from mid-2015, once the Clinical Information Systems used by healthcare providers have been upgraded with the functionality to upload these reports to your eHealth record.
My pathology page looks equally empty.
I have had SO many pathology tests! Both my endocrinologist and my rheumatologist test my thyroid function. Sometimes I have managed to co-ordinate the testing so I get one test and it gets shared to the two specialists, but that is me, the patient, doing the co-ordinating, not the doctors. I also ask for the results of tests to be sent to all three specialists and my GP – when I remember. In my view, eHealth should solve these issues. Unnecessary testing is estimated to be worth about six or seven billion dollars a year. This would sure help fight the funding “shortfall” of Medicare!
As for any actual medical information, the claims via Medicare are there too, but not much information that would be useful to a consulting specialist. If I look at the record for my last specialist appointment it says:
Consultant Physician (other than in Psychiatry) Review of Referred patient treatment and management plan – Surgery or Hospital
and gives the provider’s name. There is information about me (name, gender, age, date of birth, ID number) and not much else. In fact, it has my name, age, gender, ID number and date of birth in the header of the record and in the detail of the record. We call that data redundancy. I’m looking at my records, surely I only need to be told all that once. Even if a new doctor was looking, I think a doctor is probably smart enough to read it once and “get it”. There may be a reason for this duplication: I’d love to hear what it is! At the very least it would tell a new doctor who to contact if he needed more details, so that is something although there are no contact details for the doctor. I don’t know how many doctors have the same name, but I assume there may be more than one called Mary Jones. I tried Yellow Pages to prove my point, but couldn’t sort or filter by name. The joys of technology.
Have you ever noticed that referrals are still paper based? Dr Hespe raised the point that none of the specialists she refers to can accept electronic communication. The medical profession can do some of the most amazing things with imaging our bodies and surgical techniques have improved dramatically – but the same specialists can’t accept electronic referrals?
I can understand sharing information without a central system is difficult. Doctors work in various locations: their office, the public system, the private system, they are in theatre or on ward rounds. It is not always easy to just pick up the phone and say, “Hey Fred, we have this mutual patient….”
I expected I would be able to log on to eHealth and nominate my doctors to have access so they could all see everything. I still hope we get there. This would help break down the fragmented communication and the silos.
My son had bi-lateral de-rotation osteotomies at the Royal Children’s Hospital. The hospital has gone electronic: we have an xray and when we go upstairs to see the Professor, the xrays are on his computer screen. Yet they sent a paper letter to us to give to our GP. There is no record on eHealth that my son had this major surgery and has metal plates in both legs. I was showing the GP photos of the xrays on my phone the other day.
We have recently had endless discussions about Medicare being unsustainable. How much could we save by modernising what appears to be very outdated systems, processes and procedures? What could we achieve by eliminating some of the unnecessary red tape the doctors referred to? These are the questions we need to be asking. We need politicians with vision.
On a technical note, there are a multitude of systems involved and most of of them don’t “talk” to each, other however this is not insurmountable. It is not necessary to have real time interfaces to eHealth from the various systems in use by the many, many health providers. Most doctors (even specialists) do have their patient records on computers these days. These could be exported in a predefined format, transmitted and uploaded nightly or weekly. It is possible to achieve more detail than is currently there without massively expensive upgrades to every providers’ systems. Scandinavia can do it. Why is Australia lagging behind?
Sadly it looks as if we may now have an uphill battle to save eHealth. Pulse+IT Magazine reports momentum for the system has stalled.
Ms Powell provided a breakdown of where funds from the $140 million provided in the 2014-15 budget were allocated. $82m went to DoH to operate the system, $21.8m went to the Department of Human Services, and $2.3m to the Office of the Australian Information Commissioner. The federal government’s contribution to NEHTA for the year was $34.4m.
This isn’t a cheap system, but it does need a usability overhaul. How can we get this back on track?



{kind=link}