







eHealth and the silo culture of medicine
In February SBS Insight broadcast Saving Health. If you missed it, it is worth watching given recent Medicare funding discussions.
As a patient seeing multiple health professionals and having registered, in great hope, for eHealth, I was very interested to hear the doctors thoughts about their own profession. I understood the patients’ perspectives all too well.
There was a general consensus from the medical personnel about the silo culture of medicine in this country. As Dr Ranjana Srivastava said (in relation to repeat testing), “when doctors work in silos, you kind of don’t want to get into other people’s way”: we see this in many walks of life, not just medicine. Dr Charlotte Hespe spoke about the difficulties of getting results across barriers of fragmented communication, Dr Nick Bretland spoke of having to fax (yes, fax) forms to a public hospital to get x-ray results. I had an MRI and the films were available on my smartphone 5 minutes after the scan. Yet the GP has to fax forms to get the results? Bureaucratic red tape forms many of those barriers.
Professor John Dwyer stated ” … we do not have a patient focused health care system.” Assoc. Prof. Terry Hannan of Launceston General Hospital said, “patient centred care is the patient having their own record.”
This is where eHealth comes in. Two people in the studio audience had signed up for eHealth. TWO! Once I discovered I was unwell, I signed up for eHealth. The driver for my doing so was a very embarrassing discussion with my gastroenterologist.
“Have you had a colonoscopy before?”
“Yes, I have, years ago.”
“Who did it?”
“Ummmm, I’ve forgotten.”
“Where did you have it done?”
“Ummmm, I’ve forgotten.”
eHealth would solve that problem, nicely, wouldn’t it?
Not so much. Watching the above Insight episode, I learnt I actually have to have my GP upload some sort of summary, and according to Dr Bretland he had initially had to fill out paper forms to send in to establish his patients’ eHealth records. That will explain the scanty nature of my own eHealth record – I’ve not discussed it with my GP at all.
Candice Kriewaldt, a patient with rheumatoid arthritis, spoke of having to navigate the system herself and collate her own medical record. She highlighted the difficulties of getting medical records from one specialist to pass on to a new specialist and the problems that lead to in her treatment. I do exactly the same as Candice. I have a pretty pink folder I carry around with pathology requests pending, results, imaging CDs and details of medications.
The programme makes it reasonably clear the medical profession in Australia is still very paper based, despite the availability of technology. It appears some 4% of Australian’s surveyed expressed concerns about privacy, so eHealth is not yet where it could be or should be. May I suggest we let the 4% opt-out if they so wish and let the rest of us have our eHealth fully functional!
Here is a screen shot from my eHealth record.
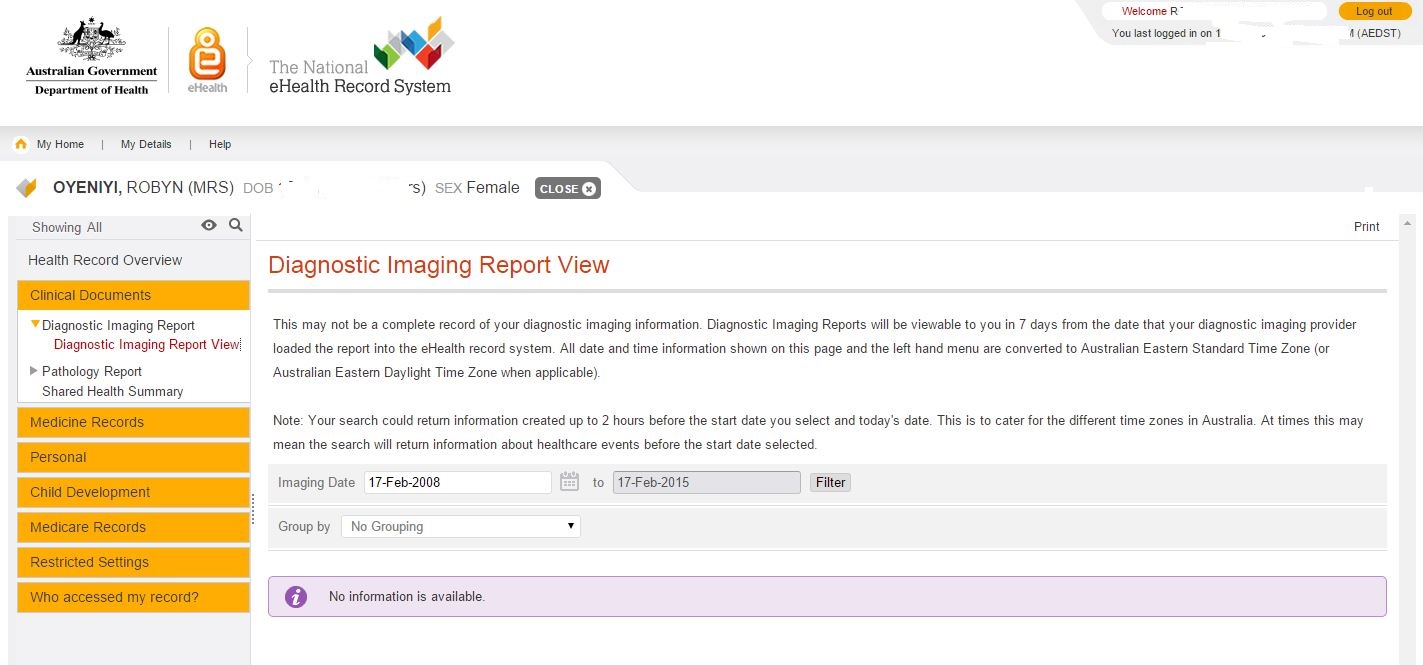
No data about my MRI
The eHealth website says:
Your eHealth record allows you and your doctors, hospitals and other healthcare providers to view and share your health information to provide you with the best possible care.
I had taken “share your health information” to mean all my recent scans and blood test results would be there. After all, I had scans available on my mobile phone five minutes after I had the scans! Surely they would be on the big fancy new eHealth web site? Well, actually, no, they are not there. I dug a little deeper into the FAQs (that means Frequently Asked Questions for the uninitiated) and found out why.
It is expected that you may start to see your pathology and diagnostic imaging reports in your eHealth record from mid-2015, once the Clinical Information Systems used by healthcare providers have been upgraded with the functionality to upload these reports to your eHealth record.
My pathology page looks equally empty.
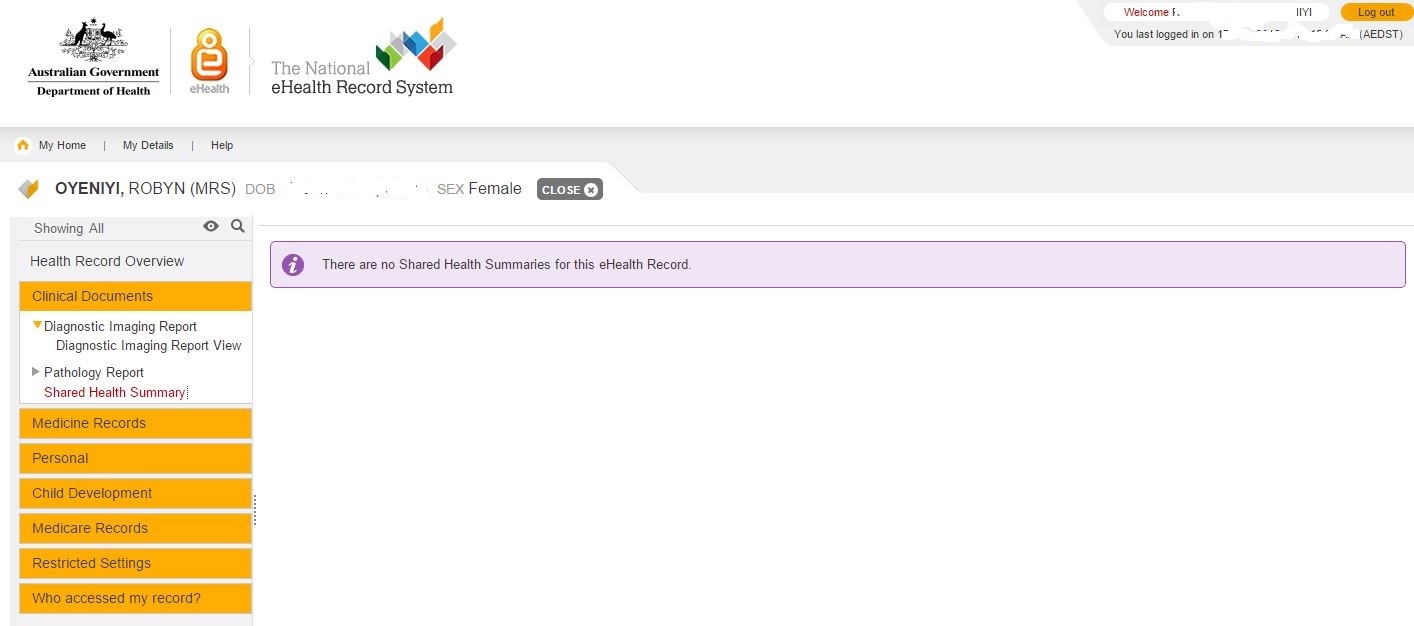
I have had SO many pathology tests! Both my endocrinologist and my rheumatologist test my thyroid function. Sometimes I have managed to co-ordinate the testing so I get one test and it gets shared to the two specialists, but that is me, the patient, doing the co-ordinating, not the doctors. I also ask for the results of tests to be sent to all three specialists and my GP – when I remember. In my view, eHealth should solve these issues. Unnecessary testing is estimated to be worth about six or seven billion dollars a year. This would sure help fight the funding “shortfall” of Medicare!
As for any actual medical information, the claims via Medicare are there too, but not much information that would be useful to a consulting specialist. If I look at the record for my last specialist appointment it says:
Consultant Physician (other than in Psychiatry) Review of Referred patient treatment and management plan – Surgery or Hospital
and gives the provider’s name. There is information about me (name, gender, age, date of birth, ID number) and not much else. In fact, it has my name, age, gender, ID number and date of birth in the header of the record and in the detail of the record. We call that data redundancy. I’m looking at my records, surely I only need to be told all that once. Even if a new doctor was looking, I think a doctor is probably smart enough to read it once and “get it”. There may be a reason for this duplication: I’d love to hear what it is! At the very least it would tell a new doctor who to contact if he needed more details, so that is something although there are no contact details for the doctor. I don’t know how many doctors have the same name, but I assume there may be more than one called Mary Jones. I tried Yellow Pages to prove my point, but couldn’t sort or filter by name. The joys of technology.
Have you ever noticed that referrals are still paper based? Dr Hespe raised the point that none of the specialists she refers to can accept electronic communication. The medical profession can do some of the most amazing things with imaging our bodies and surgical techniques have improved dramatically – but the same specialists can’t accept electronic referrals?
I can understand sharing information without a central system is difficult. Doctors work in various locations: their office, the public system, the private system, they are in theatre or on ward rounds. It is not always easy to just pick up the phone and say, “Hey Fred, we have this mutual patient….”
I expected I would be able to log on to eHealth and nominate my doctors to have access so they could all see everything. I still hope we get there. This would help break down the fragmented communication and the silos.
My son had bi-lateral de-rotation osteotomies at the Royal Children’s Hospital. The hospital has gone electronic: we have an xray and when we go upstairs to see the Professor, the xrays are on his computer screen. Yet they sent a paper letter to us to give to our GP. There is no record on eHealth that my son had this major surgery and has metal plates in both legs. I was showing the GP photos of the xrays on my phone the other day.
We have recently had endless discussions about Medicare being unsustainable. How much could we save by modernising what appears to be very outdated systems, processes and procedures? What could we achieve by eliminating some of the unnecessary red tape the doctors referred to? These are the questions we need to be asking. We need politicians with vision.
On a technical note, there are a multitude of systems involved and most of of them don’t “talk” to each, other however this is not insurmountable. It is not necessary to have real time interfaces to eHealth from the various systems in use by the many, many health providers. Most doctors (even specialists) do have their patient records on computers these days. These could be exported in a predefined format, transmitted and uploaded nightly or weekly. It is possible to achieve more detail than is currently there without massively expensive upgrades to every providers’ systems. Scandinavia can do it. Why is Australia lagging behind?
Sadly it looks as if we may now have an uphill battle to save eHealth. Pulse+IT Magazine reports momentum for the system has stalled.
Ms Powell provided a breakdown of where funds from the $140 million provided in the 2014-15 budget were allocated. $82m went to DoH to operate the system, $21.8m went to the Department of Human Services, and $2.3m to the Office of the Australian Information Commissioner. The federal government’s contribution to NEHTA for the year was $34.4m.
This isn’t a cheap system, but it does need a usability overhaul. How can we get this back on track?
10 comments
Login here Register here-
-
Lee -
Kaye Lee -
paul walter -
Robyn Oyeniyi -
Robyn Oyeniyi -
Robyn Oyeniyi -
Lee -
Fred Martin -
Robyn Oyeniyi
Return to home pagePingback: Hey doctors, here’s a new medical condition: Tough Cookie Syndrome | Love versus Goliath : A Partner Visa Journey
Professor John Dwyer is certainly correct. Our health system is not patient focused.
I don’t know what is available in other states, but there is a system in SA called OACIS for test results. It only includes results from public providers and can only be viewed by clinicians within the public hospital system. Trying to merge results from different institutions can present a challenge. Each institution has a unique patient identifier, or Unit Record Number. Patients can change their surname between presentations, making it harder to find all of their results. Patients also don’t understand the need for using their full registered name when in hospital or on medical records. Vasilios decides that he wants to be called Bill this time. Malgorzata becomes Gosia.
All of these issues that you raise highlight the importance of finding a good GP who will coordinate all of your care, especially when you have numerous problems requiring care from specialists. If you attend a clinic where you see a different GP each time, you may not get that level of care. It’s also important for people on multiple medications to have them reviewed periodically and perhaps have dosages adjusted or some medications discontinued. GPs don’t tend to do that very well and many patients are not aware that such a service exists. Although trying to convince patients to ask for a referral for this service presents its own challenges too. I’ve suggested that my mother and my partner’s mother may benefit from a medication review by a geriatrician and they won’t be in it at all.
Then there is the issue of doctor shopping. Some patients with complex problems visit different doctors so they can obtain more medication and they don’t inform each doctor of the complete list of medications they use. The scripts are also filled at different pharmacies. Since the GPs cannot detect this problem currently, some patients die to drug incompatibilities.
The lack of communication leads to untold waste on so many levels and it could be so easily fixed, but so does the arrogance of some doctors.
Pharmacists are notified of people who appear to be doctor shopping but I know of cases where the pharmacist contacts the doctor only to be told to not question them. One pharmacist was specifically instructed by the doctor that he must supply the prescription and that he did not have the qualifications to question the doctor’s decision – the patient overdosed the next day.
My son was in hospital for over two months recently. Not only did we have to fax his 12 page long discharge summary to our GP ourselves, when we went back to the hospital for outpatient care, all of the doctors had moved onto their next rotation and we had a whole new batch who weren’t interested in reading a file that was by now measured in inches. I decided to make an appointment in the rooms of the specialist who had been the consultant for his surgery. He charged my son $250 for an “initial consultation” and was also not interested in the folder of paperwork (test results etc) that we took with us.
The community nurses have been dealing with my son for 5 years and have been coming daily since he got out of hospital – they are our saviours – but they have to take photos on HIS mobile phone for us to then take to the doctor, and they spend hours on the phone trying to contact doctors when they have problems or questions or organising for equipment to be delivered or picked up.
It doesn’t need to be this hard.
I wonder if it’s not like the situation with the unemployed, or with trying to get Telstra to fix a fault. where so many bureaucratic hurdles, blockages and dead ends are placed within the system, that people give up in despair.
Then, the authorites say people wont use the so-called services and defund them.
Yes, Paul, I can see eHealth dying because no-one signs up. And we lose the benefits it could bring us.
It sure doesn’t Kaye. I thought all the doctors on the Insight programme made very valid points and clearly in many cases their hands are tied. We need to mske the whole system work for the benefit of the patients.
Very valid points Lee, especially the doctor shopping.
As for dosages, I have that all the time at the moment as we work out exactly what works and what doesn’t while keeping to the lowest effective doses of everything. Also all the doctors need to know what other doctors have given me.
Even scan timings can be important. For example one scan I had could only be done 8 weeks after the CT with dye scan I had. Yet it was only because a friend told me of the situation that I checked and made sure I had the 8 weeks between.
I just checked the latest state of play with a pharmacist. Only S8s are notified to the pharmacist immediately and only if the pharmacy is connected to Pharmaceutical Services (not sure if it has a different name in each state). Notifications are also limited to within the state.
A friend died a few years ago as a result of doctor shopping and at the inquest it was mentioned that notification to pharmacists can be months behind.
In 2004 Australia’s GDP was $466.5 billion, cost of Medicare was $8 Billion, or 1.7% of GDP. In 2014 GDP was $1560.6 Billion and cost of Medicare was $19 Billion, or 1.2% of GDP. Don’t let the Libs. fool you by quoting absolute dollar numbers, all things are relative and in relative terms cost of Medicare is actually going DOWN, or is there something wrong with my math ?
Fred, this article is not about Medicare at all. Those numbers are for the eHealth system – completely different. I know I’ve written many articles about Medicare, but this is looking at our electronic centralised medical records system.